Virus Camp
The story of the Common Cold Unit
Brian Dillon

The process begins when one of approximately 200 viruses—let us say that it is a rhinovirus, the most common of them, which accounts for between 30 percent and 50 percent of the infections in question—lights on the mucous membrane of the nose and, coaxed along by the cilia (the tiny, motile, hair-like appendages that bristle on the surface of certain cells), affixes itself to a single cell. Once absorbed by its host, the virus particle starts to replicate—within a few hours, the cell has been fatally overrun, and bursts, releasing its newborn viral cargo, which quickly seizes upon the surrounding cells. As yet, the patient feels nothing. Two days later, by which time the blood vessels of the nose have dilated at the urging of chemical messengers dispatched by besieged cells, antibodies begin to flood the affected tissues. Further chemical emissaries excite the nerve endings at the back of the nose and the top of the throat, causing the nose to run and fits of sneezing to convulse the whole area; the patient is by now too well aware of what is happening, though he or she, coming late to the chemical party that is already in full swing only centimeters from the seat of consciousness, blearily assumes that the disease has only just taken hold.
Literature has little to tell us about the progress of a cold; what narratives we have—the putting to bed, for instance, of the sodden and distraught Marianne in Jane Austen’s Sense and Sensibility—tend toward the emotionally febrile or the melancholic; they are more concerned with the metaphorical possibilities of fever, incapacity, and recovery than with the details of the disease itself. The affliction, of course, is not wholly symbolic: a cold, fever, or influenza might easily carry off a weakened constitution, while a cough might presage the specter of consumption. Still, where are the great literary accounts of the next stage in the course of a cold? The ode to blocked sinuses? The epic of catarrh? The satirical treatment of a lingering dry cough? In her essay “On Being Ill” (1930), Virginia Woolf bemoans the general omission of illness—the absence, that is, of a sustained description of the experience of being unwell—from the canon of imaginative writing. She describes what it feels like to be bedridden with a supposedly minor ailment: “‘I am in bed with influenza’—but what does that convey of the great experience; how the world has changed its shape; the tools of business grown remote; the sounds of festival become remote like a merry-go-round heard across far fields; and friends have changed, some putting on a strange beauty, others deformed to the squatness of toads, while the whole landscape of life lies remote and fair, like the shore seen from a ship at sea.” The patient, by turns elated and abject, finds that the illness elicits no sympathy for her exile from the world: “such follies have had their day; civilization points to a different goal.”
Colds and flu may have seemed more ominous in previous centuries—even since Woolf wrote “On Being Ill,” their stock of suffering has fallen dramatically, to the point where nobody will now admit to being dragged bedwards by mere aching limbs and heavy head—but they were never really numbered among the worst of torments. The common cold—and for most of its history, with only symptoms to go on, it has been impossible to tell a cold from a bout of influenza—seems to have been with us for some time: certain Egyptian hieroglyphics appear to denote the combination of a cough and a streaming nose. The Hippocratic writings speak of an excess of phlegm that leaks out through the small holes at the base of the skull, and thence to the nose, in the form of rheum. Celsus, a Roman physician of the first century AD, has this to say in his De Medicina: “[it] closes up the nostrils, renders the voice hoarse, excites a dry cough; in it the saliva is salt, there is ringing in the ears, the blood vessels of the head throb, the urine is turbid. These affections are commonly of short duration, but if neglected may last for a long while.” The notion that these symptoms were literally caused by cold or damp was established by the medicine of the Renaissance and later expressed by those, such as John Wesley, who recorded their favored treatments. In his Primitive Physick: Or, An Easy and Natural Method of Curing Most Diseases, Wesley claimed that “colds are caused by chilling because this diverts blood from the skin to the internal organs, and instead of fluid appearing as perspiration it is shed from the nose as a cold.” As a curative, Wesley advised the patient to “pare very thin the yellow rind of an orange, roll it up inside out, and thrust a roll into each nostril.”
• • •
Following a long incubation period, knowledge regarding the common cold progressed rapidly from the late nineteenth century onwards. With the discovery of bacteria, it was assumed that colds had their origin in some sort of bacteriological infection. (This led to the production of various vaccines, some of which were still in use, to no benefit at all, in the 1950s). In 1914, Dr. Walter Kruse succeeded in infecting a team of his colleagues at the Institute of Hygiene in Leipzig, using secretions from the nose of his assistant, Dr. Hilger: four of the twelve subjects caught a cold in Kruse’s first experiment, fifteen out of thirty-six in the second. With the outbreak of war, only a few months later, Kruse’s research came to an end; not, however, before he had become convinced that colds were caused not by bacteria but by a virus or viruses. The virus theory took some time to infiltrate medical opinion—in 1932, David and and Robert Thomson, in their 700-page study, The Common Cold, still adhered to the bacteriological hypothesis, and referred only fleetingly to research that pointed to a viral origin. By that time, pioneering work had been carried out at Columbia University by Dr. Alphonse Dochez, establishing that, although the type and quantity of bacteria in the nose and throat of five laboratory staff changed during the winter of 1925–26, the alterations could not be correlated with the onset of colds.
The most dedicated and long-lived research program to be devoted to this humble ailment was established near Salisbury, England, in 1946. The Common Cold Research Unit (later simply the Common Cold Unit) had its origins both in research funded in the aftermath of the influenza outbreak of 1918 (the so-called “Spanish flu”) and in the immediate exigencies and opportunities that prevailed at the outset of World War II. Between 1918 and 1919, influenza killed more people than the Great War itself; as a consequence, the Medical Research Council promoted research in the new field of virology. The work was overseen by Dr. Christopher Andrewes of the National Institute for Medical Research, who had witnessed Dochez’s experiments at Columbia and planned to replicate them in London. His funding, however, was cut during the Depression. Central to Andrewes’s research had been the question of finding suitable subjects for the experiments; in a move that predicted the methods that the CCU would use during its forty-four-year history, Andrewes recruited 100 medical students from St. Bartholomew’s Hospital: “We cannot get hold of any chimpanzees, and the next best thing to a chimpanzee is a Bart’s student.”
The immediate impetus for the establishment of the Unit came, however, from the US Army. In 1915, Harvard Medical School has sent a surgical team to Paris, and in September 1939, the university president, James B. Conant, repeated the gesture, dispatching a team from the Chemistry Department to London to study the threat of infectious disease in a country suddenly subject to vast mobilizations as troops were massed, children evacuated, and Londoners took shelter in the stations and tunnels of the Underground. The unit moved to Salisbury to become a reference laboratory in pathology, parasitology, and toxicology for the smaller hospitals in the European theater of operations. It was during this period that Andrewes conceived of a research facility expressly devoted to the common cold. On 11 February 1946, the NIMR considered Andrewes’s proposal, and a letter was sent to him regarding the question of suitable subjects for the proposed experiments: “You already know that I am not very happy about prisoners and service personnel and that I believe that free volunteers are best. There are many potential sources apart from undergraduates and I do not think we should have difficulty in getting volunteers, provided they were approached in the right way and with great enthusiasm.”
In July 1946, the first seven volunteers—all students from London—arrived at Harvard Hospital and were immediately quarantined for three days: anyone who showed symptoms of a cold during that time would have to be sent home. On this first occasion, all were given a clean bill of health and allowed to progress to the next stage of the experiment. At the NIMR in London, fluid had been obtained from the nose of Dr. Alastair Dudgeon, who had a cold: some of it was injected into the amniotic fluid of a fertile hen’s egg, in hope of growing the virus. Of the seven volunteers, three were given unadulterated fluid from Dr. Dudgeon’s nose: two of them developed colds. Neither the group of three who received the amniotic fluid, nor the one volunteer given a control solution, showed any cold symptoms. As an initial foray into the mysterious world of the virus, the experiment could be counted a success.
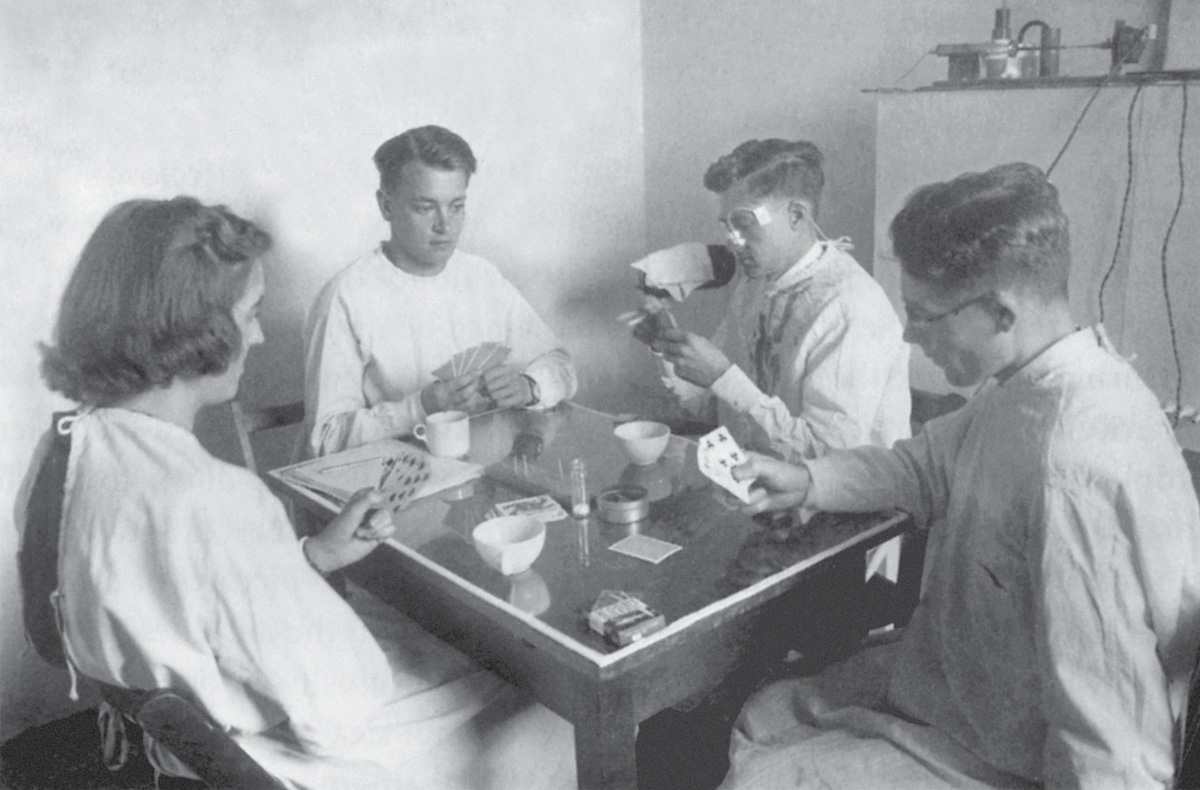
In the coming decades, the CCU subjected a steady stream of willing subjects to a wide and sometimes bizarre array of procedures, designed to ascertain the means by which a cold was transmitted. Local schoolchildren—children typically suffer from between seven and ten colds a year, while adults may experience only two to five—were invited to parties at the Unit, where adult volunteers, as yet uninfected, played games with them, or left them to amuse themselves at one end of the room while they sat behind a curtain at the other, with large fans blowing childish exhalations in their direction. James Lovelock, who would later become famous for his Gaia theory, devised a contraption that trickled fluorescent dye from the nose of a member of the lab staff who was seated, playing cards, with a group of volunteers. When the lights were turned off, the dye was found on the cards, the table, the fingers of the players, and other, surprisingly far-flung, parts of the room. (It remained unclear, however, how the real thing might infiltrate the noses of the volunteers and thus transmit a cold.) In order to discover just how infectious the product of a sneeze might be, the volunteers’ heads were enclosed in large plastic bags, and their noses tickled until they sneezed: the air was sucked out and its particles collected using a device called a Porton Impinger. In a reversal of the same procedure, the volunteer sat on a chair inside a wardrobe (left behind by the American forces) while virus suspension was sprayed through a hole above his head.
Unsurprisingly, the Unit attracted a number of cranks, quacks, and hypochondriacs, though not, it seems, among the volunteers. It was common for members of the public to write seeking advice about catarrh, sinus trouble, nasal polyps, and allergies, but also to offer their own recipes for treatments and cures. A predictable number of the latter involved some sort of hot, sweet drink, generously laced with alcohol. Garlic, too, was recommended: it was either to be eaten in large quantities or, less conventionally, placed in one’s socks. One correspondent wrote to inform the experts that he had been successfully treating his own colds for thirty years by inserting a blob of antiseptic cream into each nostril as soon as he felt the first symptoms. As yet, he lamented, his family had declined to follow his perfectly sensible regimen.
The singular oddity of the Unit itself, however, and the reason it became, during its four and a half decades, a regular subject of media interest in Britain, was its reliance on volunteers recruited from the general public. It is difficult now, in an era when public trust in medical and scientific institutions is at a low ebb, to quite grasp the mixture of curiosity, civic-mindedness, and boredom that motivated those who elected to spend ten days (often, in other words, their whole allotted annual holiday) in the austere military huts that comprised the facility at Salisbury. At first, the standards of accommodation, heating, and food would actually have been something of an improvement on the everyday conditions of many in war-weary Britain. But as the country recovered, and the memory of wartime duty receded, or became the object of fond satire, something of that sense of doing one’s bit for one’s country survived into the era of television and foreign holidays.
In his book Cold Wars: The Fight Against the Common Cold (2002), David Tyrrell, the Unit’s director from 1957 until its closure in 1990, records the favorable accounts written by volunteers in the first years of the CCU’s operation. An early visitor, a male teacher, recalled: “It was a fine place. I was able to retreat in the monastic sense, once to read, the second time to revise for an impending examination. Everything was gently controlled and, although the Scottish matron was somewhat unnerving and terrifying, the lack of authority, apart from the very few things we were forbidden, was a good relaxation after a heavy term of teaching. And I was given a cold on neither visit.” One woman, also a teacher, volunteered six times in eleven years: “Time flew, sewing, reading, going on the occasional walk. It was a complete break from the world, a time to return to the freedom of childhood without its restraints. The yellow trolley (bringing meals) was a highlight of the trials. Pavlov’s dogs had nothing on us.”
Despite these memories of childish liberation, the quotidian lives of the volunteers were necessarily constrained. They were housed in pairs or in threes, in huts that contained a sitting room, bedrooms, medical room, and a small kitchen. Each pair or trio had to stay thirty feet from those in the neighboring huts—it was possible to shout between huts, but even the chattiest soon tired of this. Later, a telephone exchange was installed, and volunteers could pass the evenings playing chess by phone with their neighbors. Unless married, men and women were housed separately: one young couple managed to convince the authorities to let them go for a walk together in the countryside, with a taut thirty-foot rope between them; but they soon walked either side of a tree and were forced together. Tyrrell’s account of such capers reads much like the memoir of an indulgent boarding-school headmaster, and a little like the plot of one of the medical comedies (the Doctor… and Carry On… series) that were popular with British cinema-goers in the postwar period. He writes of one man, initially attracted by an advertisement at Dover town hall, and who returned another nine times: “On one occasion he developed a romantic feeling for a woman volunteer, an oboist who played with a London orchestra. ‘I had brought my guitar down with me,’ he said, ‘and we played duets at 30 feet while the trial lasted, and closer at the end.’”
• • •
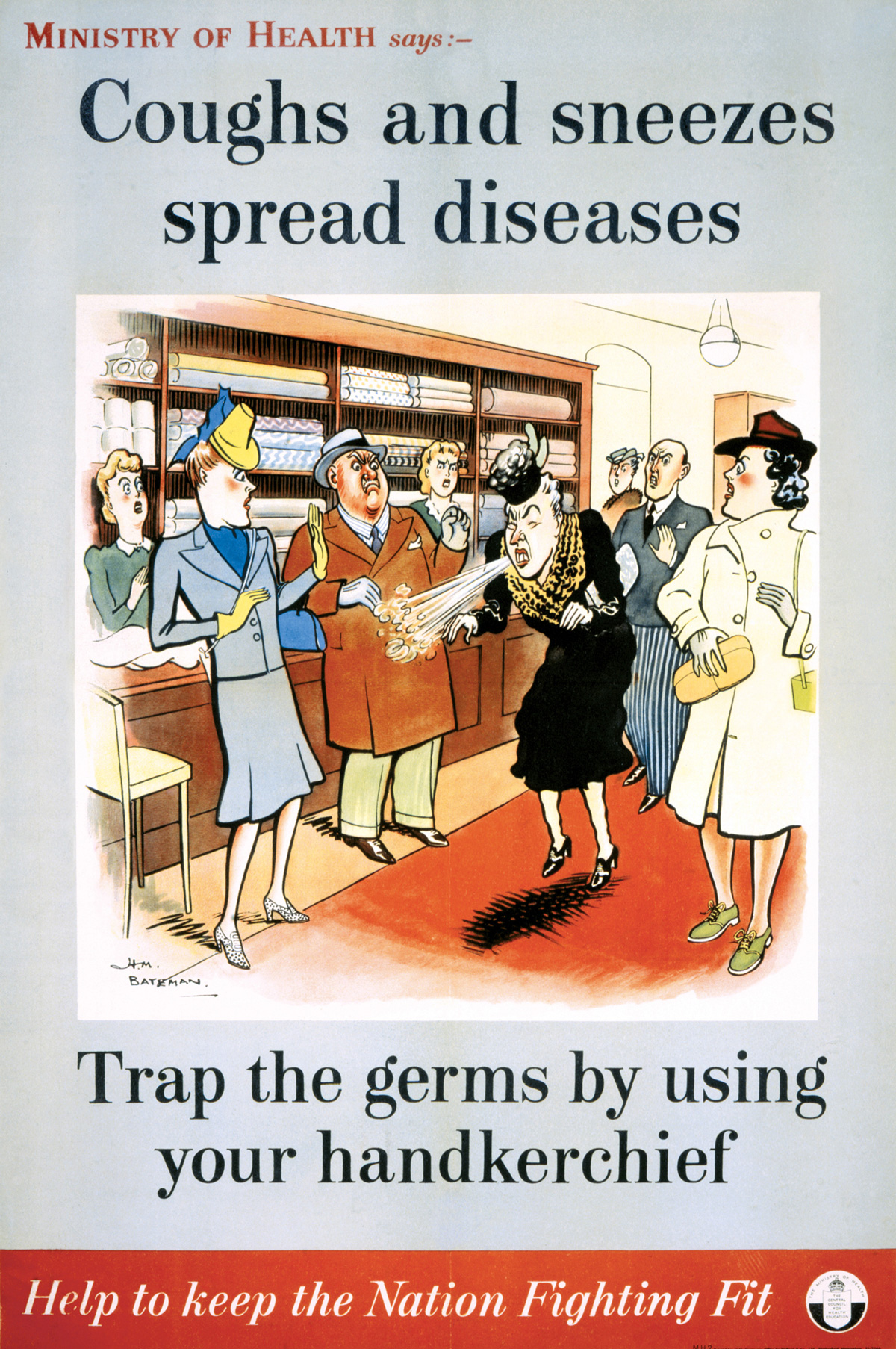
The main thrust of the Unit’s research was always to discover how colds and flu were transmitted, and only secondarily to treat them. Although several strands of inquiry were devoted, especially in later years, to treatment—antihistamines, Vitamin C, antibiotics, and interferon were all canvassed as potential cures: none of them worked—the CCU remained a product of a particular wartime mentality, and the fear of contagion that came with it. A cure for the common cold was low on the list of priorities precisely because the Unit was born not out of concern for the suffering of those briefly afflicted with a cold, but from a concern for their productivity. The somewhat infantilizing culture of the CCU is entirely of a piece with a campaign launched by the Ministry of Health in 1942, designed to appraise the public of the effect on the war effort of even minor infections. A series of posters was commissioned from the cartoonist H. M. Bateman: each bore the legend, “Coughs and sneezes spread diseases. Trap the germs by using your handkerchief. Help to keep the Nation Fighting Fit.” A succession of feckless sneezers was depicted, in the queue at a canteen, in the middle of a crowded cinema, at the production line of a munitions factory—each red-faced offender surrounded by outraged individuals.
In 1945, a short film was produced to drive the message even further home. It showed a middle-aged man, liberally sneezing in public without a handkerchief, and responding, confusedly at first, to the authoritative tones of the voiceover: “Hi! Stop it, you. Stop it. STOP IT. Come here. What do you think you’re up to? You’ve probably infected thousands of people already. What do you think this is for?” At which point a disembodied hand is thrust under his nose, proffering a pristine, folded, white handkerchief.
The CCU, in other words, was the peacetime continuation of a condition of mind fostered during a state of emergency. It is perhaps best understood as a vision of medical progress that was conjured into being by scientists and the military, but sustained by a British public that was keen to retain, for a time, a sense of order, duty, and civic self-sacrifice that was otherwise slipping away. One might say that its quarantines and thirty-foot exclusion zones functioned as a set of consoling metaphors for the more alarming prophylaxis of nuclear deterrence. The fight against the rhinovirus was a synecdoche for the wider but no more intricate effort to keep a new enemy at bay: its existence assured the populace of the essential benignity of the scientific and military machinery of the other Cold War. The volunteers who answered the advertisements that were regularly placed in national newspapers and magazines constituted a sort of sniffling civil defense force: as much against public skepticism of such official facilities as against the virus itself. It was, no doubt (in whatever minor a way), of some benefit to successive British governments to have such a ready symbol of the conjunction of militarism and state-run medicine, especially one that seemed, in the popular imagination, both useful and somewhat absurd.
This did not stop persistent rumors that the Common Cold Unit was in fact a covert adjunct to the nearby Defence Science and Technology Laboratory at Porton Down, on the other side of the town of Salisbury. The two facilities shared equipment and data, especially in the 1950s and 60s. The link continues to trouble the Department of Defence, after an inquest in 2004 found that a 1953 sarin toxicity test at Porton Down, in which an airman, Ronald Maddison, aged 20, died, had been illegal. Maddison’s family had asserted that he had believed he was taking part in an experiment to find a cure for colds: a claim still refuted by the Department of Defence, which denies that any volunteers, civilian or enlisted, were ever subjected to biochemical agents while under the impression that they were part of the struggle against an ancient and recalcitrant, if mostly just annoying, enemy.
Brian Dillon is UK editor of Cabinet, and writes regularly for Frieze, Modern Painters, and Art Review. His memoir In the Dark Room (Penguin) won the inaugural Irish Book Awards non-fiction prize, 2006. He is working on Tormented Hope: Nine Hypochondriac Lives, to be published in 2008.
Spotted an error? Email us at corrections at cabinetmagazine dot org.
If you’ve enjoyed the free articles that we offer on our site, please consider subscribing to our nonprofit magazine, which includes unlimited access to all our archives.